
Itching and Elevated Liver Enzymes: Causes, Treatments, and When to Seek Medical Attention
What causes itching and elevated liver enzymes. How are these symptoms treated. When should you consult a doctor for itching and elevated liver enzymes. What are the potential complications of untreated liver-related itching.
Understanding the Link Between Itching and Liver Disease
Itching, or pruritus, is a common symptom associated with chronic liver diseases. While not everyone with liver disease experiences itching, it can be a significant concern for those who do. The itching may be localized to a specific area or present as an all-over sensation, often leading to an overwhelming urge to scratch.
Elevated liver enzymes are often detected through blood tests and can indicate liver damage or inflammation. When these two symptoms occur together, it’s crucial to understand their potential connection and implications for overall health.
Which Liver Conditions Are Most Commonly Associated with Itching?
Itching is most frequently observed in the following liver conditions:

- Primary biliary cirrhosis (PBC)
- Primary sclerosing cholangitis (PSC)
- Intrahepatic cholestasis of pregnancy
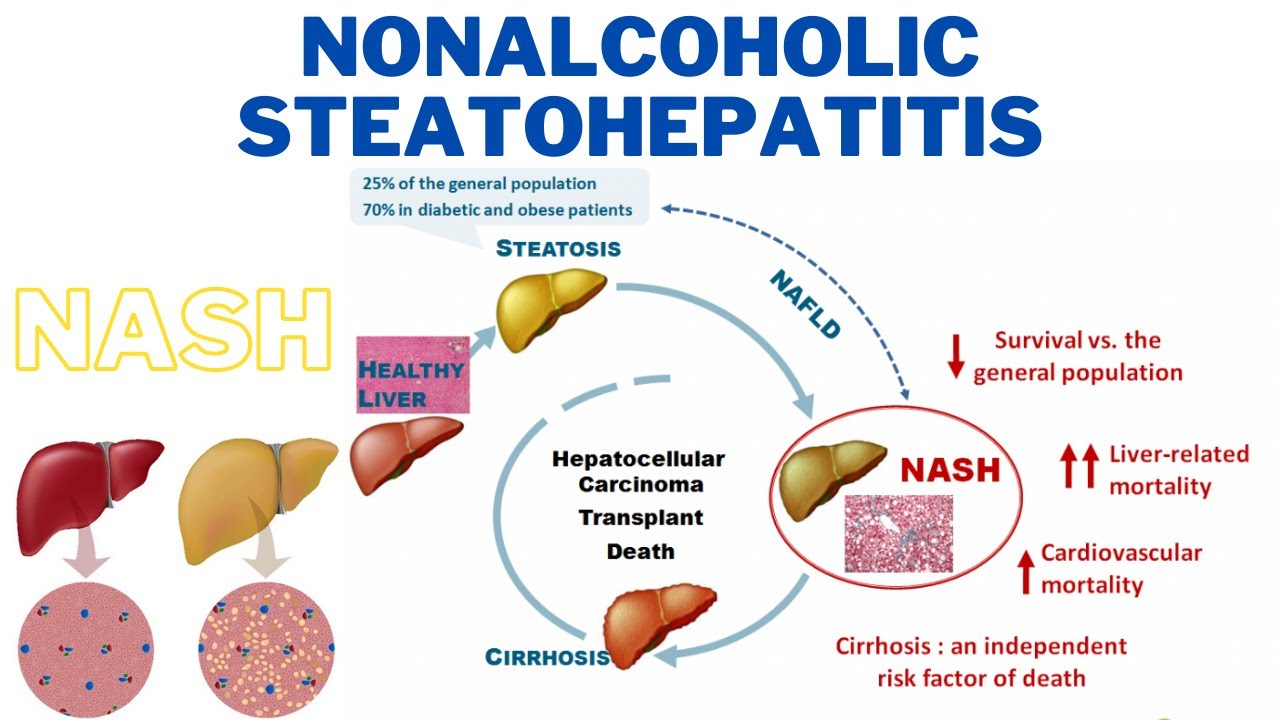
Interestingly, pruritus is less common in alcohol-related liver diseases and nonalcoholic fatty liver diseases. This distinction can provide valuable information for healthcare providers when diagnosing and treating liver conditions.
Potential Causes of Liver-Related Itching
Despite extensive research, scientists have yet to identify a single substance responsible for itching in liver disease. It’s likely that a combination of factors contributes to this symptom. Here are some potential causes under investigation:
Bile Salt Accumulation
In liver disease, higher levels of bile salts can accumulate under the skin, potentially causing itching. However, it’s important to note that not everyone with elevated bile salt levels experiences itching, and some individuals feel itchy despite normal bile salt levels.
Histamine Levels
Some individuals with pruritus have elevated histamine levels. Curiously, antihistamines are not typically effective in treating liver-related itching, suggesting that other mechanisms may be at play.

Serotonin’s Role
Serotonin may alter itch perception, which could explain why selective serotonin reuptake inhibitors (SSRIs) can help manage pruritus in some people with liver disease.
Hormonal Influences
Female sex hormones may exacerbate itching, as some individuals experience worsened symptoms during pregnancy or while undergoing hormone replacement therapy.
Serum Alkaline Phosphatase (ALP)
Elevated levels of ALP are often observed in individuals experiencing liver-related itching, suggesting a potential connection between this enzyme and pruritus.
Lysophosphatidic Acid (LPA) and Autotaxin
People with itching and liver disease may have higher levels of LPA, which affects numerous cellular functions. Autotaxin, an enzyme involved in LPA formation, may also play a role in liver-related pruritus.
Managing Liver-Related Itching: Treatment Options and Self-Care Strategies
Itching caused by liver disease is unlikely to improve on its own, but various treatment options are available. Due to the complex nature of liver-related pruritus, a combination of therapies may be necessary, and some trial and error might be involved in finding the most effective approach.
Avoiding Scratch-Induced Complications
One of the most critical aspects of managing liver-related itching is resisting the urge to scratch. Excessive scratching can lead to skin damage, increasing the risk of infection and further complications. Consider these strategies to minimize scratching:
- Keep fingernails short to reduce the likelihood of breaking the skin if scratching occurs
- Cover itchy areas with clothing to reduce temptation
- Wear gloves at night if you tend to scratch during sleep
Skin Care and Environmental Modifications
Implementing proper skin care routines and making environmental adjustments can help alleviate itching and prevent skin irritation:
- Use lukewarm or cool water for bathing instead of hot water
- Limit time spent in hot environments or direct sunlight
- Choose mild, fragrance-free soaps and moisturizers
- Apply cold, wet compresses to itchy areas
- Avoid known skin irritants and harsh chemicals
- Wear loose-fitting, breathable clothing
- Use a humidifier during dry seasons to maintain skin hydration
Topical Treatments for Localized Itching
For mild, localized itching, several over-the-counter (OTC) topical treatments may provide relief:

- Aqueous cream with 1% menthol
- OTC corticosteroid creams
- Calcineurin inhibitors
It’s essential to follow label directions and inform your healthcare provider about any OTC treatments you’re using.
Prescription Medications for Liver-Related Itching
When OTC treatments and self-care strategies prove insufficient, your physician may recommend prescription medications to manage liver-related itching:
Cholestyramine (Prevalite)
This oral medication helps remove bile salts from circulation, potentially reducing itching in individuals with liver disease.
Rifampicin (Rifadin)
While primarily used as an antibiotic, rifampicin has shown effectiveness in managing pruritus associated with liver conditions.
Sertraline
As an SSRI, sertraline may help alleviate itching by modulating serotonin levels and itch perception.
Naltrexone
This opioid antagonist has demonstrated efficacy in reducing itching intensity in some individuals with liver disease.
When to Seek Medical Attention for Liver-Related Itching
While occasional mild itching may not be cause for immediate concern, persistent or severe itching, especially when accompanied by other symptoms, warrants medical evaluation. Consider seeking medical attention if you experience:
- Intense, unrelenting itching that interferes with daily activities or sleep
- Itching accompanied by jaundice (yellowing of the skin or eyes)
- Unexplained weight loss or fatigue
- Abdominal pain or swelling
- Dark urine or pale stools
- Signs of skin infection due to scratching
Early intervention can help manage symptoms more effectively and prevent potential complications associated with liver disease.
Diagnostic Approaches for Liver-Related Itching
When evaluating liver-related itching, healthcare providers may employ various diagnostic tools and tests to determine the underlying cause and assess liver function:
Blood Tests
Comprehensive blood panels can provide valuable information about liver function and potential causes of itching:
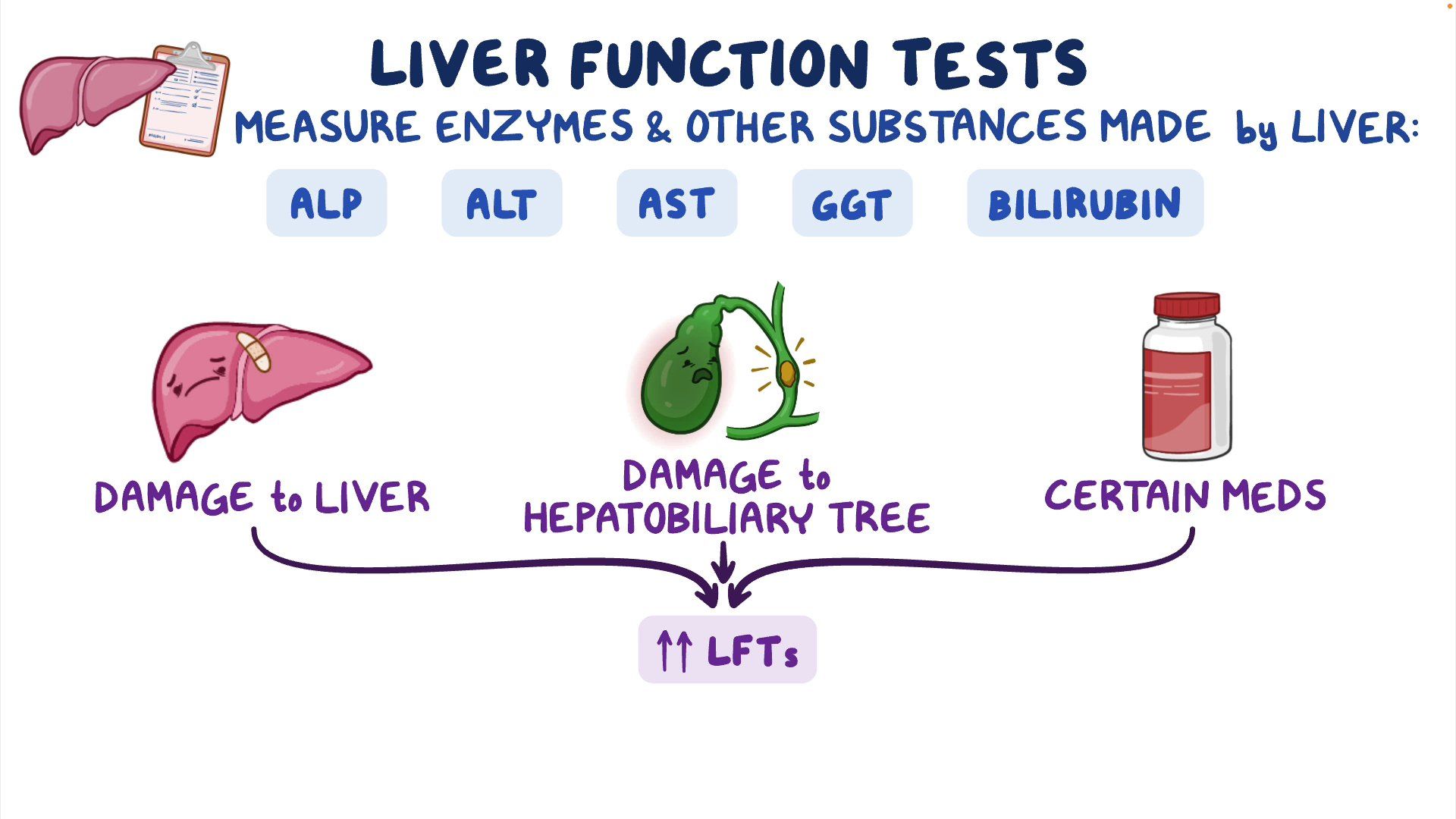
- Liver enzyme tests (ALT, AST, ALP, GGT)
- Bilirubin levels
- Complete blood count (CBC)
- Bile acid levels
- Autoimmune markers
Imaging Studies
Imaging techniques can help visualize the liver and surrounding structures:
- Ultrasound
- CT scan
- MRI
Liver Biopsy
In some cases, a liver biopsy may be necessary to confirm a diagnosis or assess the severity of liver disease.
Potential Complications of Untreated Liver-Related Itching
While itching itself may not directly cause severe health issues, it can lead to various complications if left untreated:
Skin Damage and Infection
Persistent scratching can break the skin, increasing the risk of bacterial infections. In severe cases, this can lead to cellulitis or other skin infections requiring medical intervention.
Sleep Disturbances
Intense itching can significantly disrupt sleep patterns, leading to fatigue, irritability, and decreased quality of life. Chronic sleep deprivation can also have broader health implications, affecting cognitive function and overall well-being.
Psychological Impact
Persistent itching can take a toll on mental health, potentially leading to anxiety, depression, or other psychological distress. The constant discomfort and visible skin changes may also affect self-esteem and social interactions.
Progression of Liver Disease
While itching itself doesn’t necessarily indicate worsening liver function, ignoring this symptom may lead to delayed diagnosis and treatment of underlying liver conditions. Prompt medical attention is crucial for managing liver disease effectively and preventing its progression.
Lifestyle Modifications to Support Liver Health
In addition to managing itching symptoms, individuals with liver disease can benefit from lifestyle changes that support overall liver health:
Dietary Adjustments
A liver-friendly diet can help manage symptoms and support liver function:
- Reduce sodium intake to prevent fluid retention
- Limit processed foods and saturated fats
- Increase consumption of fruits, vegetables, and whole grains
- Stay hydrated with water and herbal teas
- Avoid alcohol and limit caffeine intake
Regular Exercise
Moderate physical activity can help improve liver function and reduce symptoms:
- Aim for at least 30 minutes of moderate exercise most days of the week
- Consider low-impact activities like walking, swimming, or yoga
- Consult with your healthcare provider before starting a new exercise regimen
Stress Management
Chronic stress can exacerbate liver disease symptoms. Implement stress-reduction techniques such as:
- Meditation or mindfulness practices
- Deep breathing exercises
- Progressive muscle relaxation
- Engaging in hobbies or activities you enjoy
Avoiding Hepatotoxic Substances
Protect your liver by avoiding substances that can cause further damage:

- Limit or avoid alcohol consumption
- Be cautious with over-the-counter medications, especially acetaminophen
- Avoid exposure to environmental toxins when possible
By implementing these lifestyle modifications alongside medical treatments, individuals with liver-related itching can improve their overall health and potentially reduce the severity of their symptoms.
Causes, Treatment, When to See a Doctor
We include products we think are useful for our readers. If you buy through links on this page, we may earn a small commission Here’s our process.
Healthline only shows you brands and products that we stand behind.
Our team thoroughly researches and evaluates the recommendations we make on our site. To establish that the product manufacturers addressed safety and efficacy standards, we:
- Evaluate ingredients and composition: Do they have the potential to cause harm?
- Fact-check all health claims: Do they align with the current body of scientific evidence?
- Assess the brand: Does it operate with integrity and adhere to industry best practices?
We do the research so you can find trusted products for your health and wellness.
Read more about our vetting process.
Was this helpful?
Itching is a common symptom of chronic liver diseases. Treatment options include avoiding scratching, using mild soaps, applying topical creams, taking prescription oral medications, and more.
Itching (pruritus) is one symptom of chronic liver disease, though not everyone with liver disease develops it.
You might have a localized itch, such as on your lower arm, or it might be an all-over itch. Either way, it can lead to a distracting, often overwhelming, desire to scratch.
A little itch now and then is no cause for concern. But continual itching can interfere with sleep and lead to a host of other problems. When that happens, it becomes a serious health concern.
In this article, we’ll explore the causes of itching in liver disease, why you should see your doctor, and how to find relief.
Pruritus is rare in alcohol-related liver diseases and nonalcoholic fatty liver diseases. It’s most commonly associated with:
- primary biliary cirrhosis (PBC)
- primary sclerosing cholangitis (PSC)
- intrahepatic cholestasis of pregnancy
Some experimental and clinical studies have been done, but scientists have yet to identify a single substance responsible for itching in liver disease. It may be that it’s caused by a combination of factors.
It may be that it’s caused by a combination of factors.
Here are some of the possibilities researchers are looking into:
- Bile salts. If you have liver disease, you might have higher levels of bile salt accumulating under the skin, which may cause itching. Not everyone with high levels of bile salts feel itchy, and some people feel itchy despite a normal bile salt level.
- Histamine. Some people with pruritus have raised histamine levels. Antihistamines aren’t usually effective in treating it, though.
- Serotonin. Serotonin may alter itch perception. That may be why selective serotonin reuptake inhibitors (SSRIs) can help manage pruritus in some people.
- Female sex hormones. Itching sometimes gets worse during pregnancy or if you’re undergoing hormone replacement therapy.
- Serum alkaline phosphatase (ALP).
 People with itch related to liver disease may have elevated ALP.
People with itch related to liver disease may have elevated ALP. - Lysophosphatidic acid (LPA) and autotaxin (an enzyme forming LPA). LPA affects many cellular functions. People with itching and liver disease may have higher levels of LPA.
 People with itch related to liver disease may have elevated ALP.
People with itch related to liver disease may have elevated ALP.Itching caused by liver disease probably won’t improve on its own, but it can be treated.
Because the causes aren’t totally understood, it’s hard to say which treatment might work for you. It may take a combination of therapies along with a certain amount of trial and error.
Avoid scratching
It’s important to avoid scratching that itch because it can make matters much worse. Keep your fingernails short so that if you do scratch, you’re less likely to break the skin and open the door to infection.
If you find yourself scratching too much, try to avoid temptation by keeping your skin covered. If you tend to scratch a lot during the night, wear gloves to bed.
Here are some other things you can do to prevent skin irritation and ease itching:
- Use warm or cool water rather than hot water for showers and baths.
- Try not to spend too much time in hot environments or in the sun.
- Choose mild soaps that don’t contain added fragrances.
- Use gentle, fragrance-free moisturizers to combat dryness.
- Apply a cold, wet cloth to the itchy area until the urge to scratch eases up.
- Avoid substances or materials that irritate your skin.
- Wear gloves when using harsh products.
- Wear loose-fitting, breathable clothing.
- Use a humidifier during the dry winter months.

Shop for a humidifier online.
Apply anti-itch topicals
If you have a mild, localized itch, you can try aqueous cream with 1 percent menthol. Other over-the-counter (OTC) topicals, such as corticosteroids and calcineurin inhibitors, may also improve itching.
Follow label directions and be sure to tell your doctor you’re using them.
Find corticosteroid creams online.
Take prescription oral medications
Your physician may recommend oral treatments, such as:
- Cholestyramine (Prevalite). This oral medication helps remove bile salts from circulation.
- Rifampicin (Rifadin). This medication inhibits bile acids. Taken daily, it requires regular monitoring due to the potential for serious side effects such as hepatitis or renal impairment.
- Naltrexone (Vivitrol). Taken daily, this medication blocks the effects of opioids. It requires regular monitoring.
- Sertraline (Zoloft). This SSRI is also taken daily. It’s usually prescribed as an antidepressant. Other antidepressants, such as fluoxetine (Prozac), may also be used to treat chronic itch.
 This oral medication helps remove bile salts from circulation.
This oral medication helps remove bile salts from circulation.Try antihistamines (for sleep)
Antihistamines haven’t been shown to be effective in treating itch caused by liver disease, though they may help you fall asleep despite the itch.
Consider light therapy
Another option is light therapy, also known as phototherapy. This treatment exposes the skin to specific types of light to promote healing. It can take several sessions to start working.
It can take several sessions to start working.
Discuss a liver transplant with your doctor
When treatment doesn’t work and quality of life is severely affected, your doctor may want to discuss the possibility of a liver transplant. This may be an option even if your liver is still functioning.
Liver failure is sometimes accompanied by itching. But you can develop problem itching early on, before you even know you have liver disease.
In fact, pruritis can develop at any point in liver disease. This symptom alone says nothing about liver disease severity, progression, or prognosis.
That doesn’t mean it’s not a serious problem. When itching persists, it can contribute to:
- insomnia
- fatigue
- anxiety
- depression
- impaired quality of life
Itching associated with liver disease tends to be worse in the late evening and during the night. Some people may itch in one area, such as a limb, the soles of their feet, or the palms of their hands, while others experience an all-over itch.
Itching linked to liver disease doesn’t generally involve rash or skin lesions. However, you can develop visible irritation, redness, and infection due to excessive scratching.
The problem can be exacerbated by:
- exposure to heat
- stress
- menstruation
- pregnancy
- hormone replacement therapy
Because there are so many things that cause itchy skin, it’s possible that itching isn’t related to your liver disease.
A severe case of dry skin (xerosis cutis) can certainly lead to troublesome itching. Itching without rash can also be a side effect of certain medications, including opioids, statins, and blood pressure drugs.
Skin conditions such as eczema and psoriasis cause itching accompanied by inflamed, red, or scaly skin.
Skin itching can be due to an allergic reaction to such things as:
- poison ivy
- cosmetics
- soaps
- household cleaning products
- chemicals
- fabrics like wool or mohair
In addition to itching, an allergic reaction is likely to involve skin redness, rash, or hives.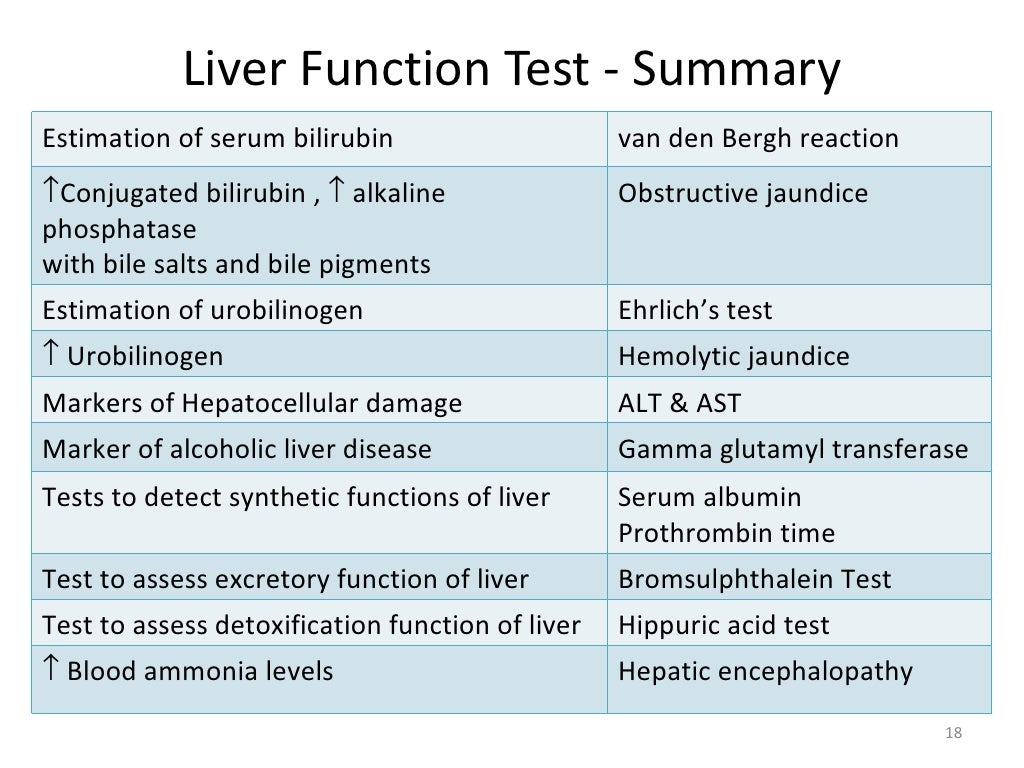
Other diseases and disorders that can lead to itchy skin include:
- anxiety
- depression
- diabetes
- iron deficiency anemia
- kidney failure
- leukemia
- lymphoma
- multiple myeloma
- multiple sclerosis (MS)
- obsessive-compulsive disorder (OCD)
- pinched nerve
- shingles (herpes zoster)
- thyroid problems
Itching is also associated with:
- bacterial, viral, fungal, or parasitic skin infection
- insect bites or stings
- pregnancy
It’s not always possible to determine the cause of itching.
If you have liver disease, see your doctor whenever you have new or worsening symptoms. That includes itching.
While it may not mean anything as far as disease progression or prognosis are concerned, you won’t know that for certain without a thorough examination.
It’s especially important to tell your doctor if you’re having trouble sleeping and if the itching is affecting your quality of life.
Itching associated with liver disease may be due to a variety of factors. Severe itching can lead to a host of other issues, so it’s important to see your doctor for diagnosis and treatment.
Liver disease progression and other causes
Itchy skin, or pruritus, can be a symptom of liver disease. However, not everyone with liver disease experiences itching, and the specific causes of this itching are unknown.
This article looks at the possible causes of itching in people with liver disease and other possible causes of itching. We also cover how to treat it and when to speak with a doctor.
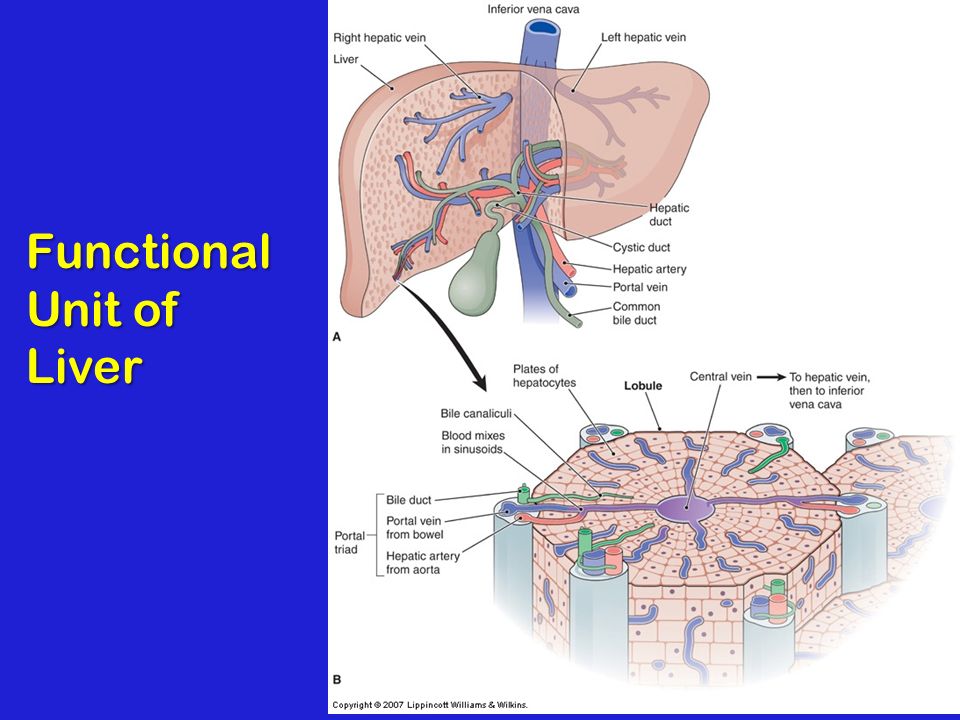
The liver is the body’s largest solid organ. It breaks down fats, detoxifies the body, produces cholesterol and proteins, and stores vitamins.
The Centers for Disease Control and Prevention (CDC) state that 4.5 million adults in the United States have a diagnosis of liver disease.
Some types of liver disease that involve itching include:
- primary biliary cirrhosis (PBC)
- intrahepatic cholestasis of pregnancy
- chronic hepatitis B and C
- familial intrahepatic cholestasis
- Alagille syndrome
- primary sclerosing cholangitis (PSC)
- cancer of the head of the pancreas
- biliary obstructive disease
Itching is also more common with autoimmune liver diseases, such as PSC and PBC, and overall with intrahepatic liver diseases, which refers to conditions affecting structures inside the liver.
In contrast, extrahepatic liver diseases affect the liver but occur outside the organ. Some of these can involve itching, such as PSC and cancer of the head of the pancreas.
Pruritus is less common with alcohol-induced liver diseases and nonalcoholic fatty liver disease.
Scientists do not know precisely why itching occurs with liver disease. Below are some theories that scientists have been investigating.
Bile salts
The authors of a 2015 research article suggest that liver disease can increase the levels of bile salts, which then gather under the skin, resulting in pruritus. The body makes bile salts from bile acids.
However, itching does not affect everyone with liver disease and high levels of bile salt, and scientists have not confirmed a link between the severity of pruritus and bile salt concentration.
Other research suggests that unusual levels of bilirubin stimulate peripheral itch sensory neurons. Bilirubin is a pigment of bile. People with liver disease often have high levels of bilirubin.
Other naturally occurring chemicals
Other substances that occur naturally in the body may trigger pruritus, according to some research.
They include:
- histamine
- opioids
- serotonin
- female sex hormones
Histamine levels tend to be higher in people with cholestatic pruritus, although itching does not appear to be worse in individuals with higher histamine levels.
Some believe that serotonin can alter a person’s itch perception, resulting in increased itching. Some people have found that taking serotonin reuptake inhibitors helps manage pruritus. Those who took opioid antagonists also reported that their itching improved.
Sensitive skin cells
In 2021, some researchers found evidence that itching with PBC might involve a nerve reaction in keratinocytes, cells in the skin’s outer layer.
People with PBC have high levels of a lipid (fat) known as lysophosphatidylcholine (LPC) circulating in their blood. When the scientists injected the skin of mice with this substance, they noted an increase in itching.
When the scientists injected the skin of mice with this substance, they noted an increase in itching.
They concluded that as LPC reaches the skin through circulation, it may trigger a reaction that leads to itching.
Many other causes of itchy skin do not relate to the liver.
These include:
- atopic eczema
- psoriasis
- dry skin
- heat rash
- allergies
- hives
- fungal infections, such as thrush, ringworm, and athlete’s foot
- parasitic infections, for instance, scabies and lice
- hormonal changes, for example, during pregnancy and around menopause
- other health conditions, such as thyroid or kidney problems
Scientists do not know why itching occurs with liver disease. They believe some chemicals in the body may play a role, but there is no apparent link between the levels of these chemicals and the severity of itching.
This suggests that, as far as doctors know, itching does not indicate that liver disease is worsening, at least for some liver conditions.
Theories to explain why the itching intensity varies focus on the nature of the nerve pathways that carry the feeling or perception of itching.
In one theory, the same pathways carry both itch and pain stimuli. In other, they are separate. In this case, genetic, dietary, and environmental factors may play a role.
Researchers have investigated various possible treatments for itching due to liver disease. However, there is no certain way of treating it, as doctors do not yet know why it occurs.
Prescription drugs that may help manage symptoms include:
- bile acid sequestrants, such as cholestyramine (Prevalite)
- bile acids that help the body remove other bile acids, for instance, ursodeoxycholic acid
- rifampicin (Rifadin), an antibiotic
- opioid inhibitors, such as naloxone (Narcan) and naltrexone (Vivitrol)
- a serotonin receptor antagonist called sertraline (Zoloft)
However, some of these treatments can have adverse effects.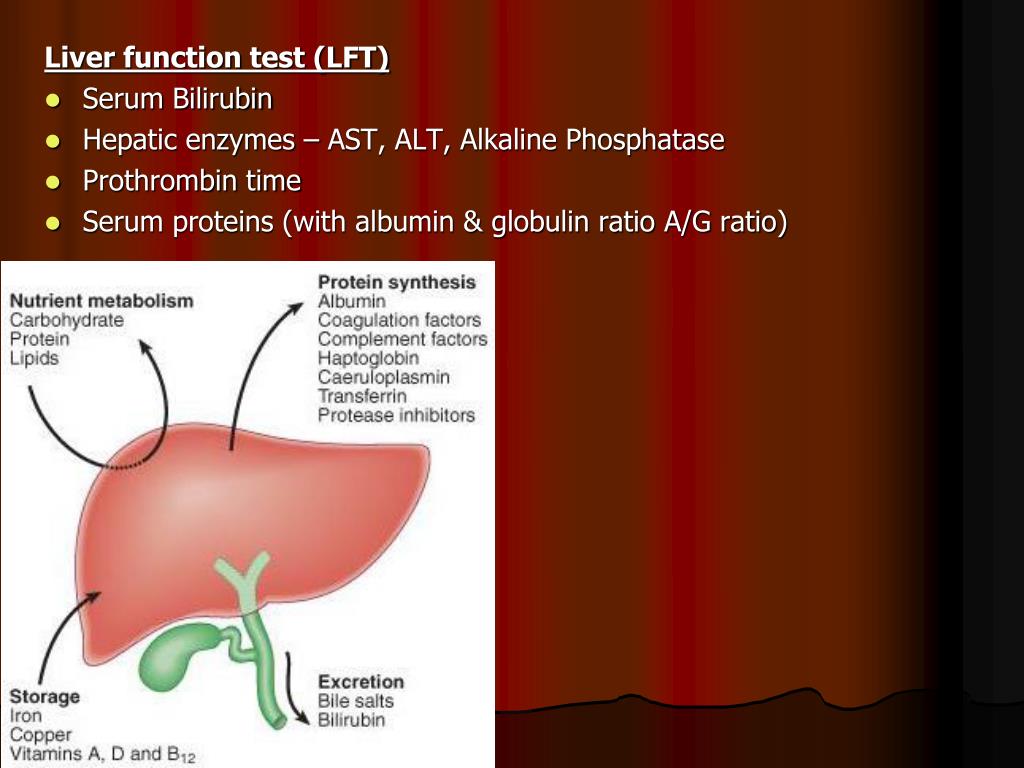 With this in mind, scientists continue to investigate other options.
With this in mind, scientists continue to investigate other options.
Another treatment possibility may be antihistamines, although an older review from 2010 concluded that topical antihistamines were ineffective.
Home remedies
Here are some other tips for reducing symptoms:
- applying skin moisturizers
- avoiding irritants, such as perfumed cosmetics
- taking cool baths
- applying a cold, wet cloth to affected areas
- avoiding hot environments
- wearing loose-fitting clothing
- avoiding scratching where possible
- wearing gloves when sleeping to avoid scratching
- using an aqueous cream with 1% menthol to soothe and cool the skin
Itchy skin is typically harmless, but it can sometimes indicate liver disease.
Often, liver disease does not have any symptoms in the early stages. However, a person should speak with a doctor if they experience:
- yellowing of the whites of the eyes, a sign of jaundice
- fatigue and weakness
- a loss of appetite, which may lead to weight loss
- a loss of libido, or sex drive
- nausea or vomiting
A person may also wish to seek medical advice if itching:
- is severe or persistent
- affects the whole body
- leads to excessive scratching, resulting in secondary skin lesions or infection
- occurs on the soles of the feet and palms of the hands
- disturbs their sleep
- affects their quality of life
People with an existing diagnosis of liver disease who experience itching may wish to seek medical advice.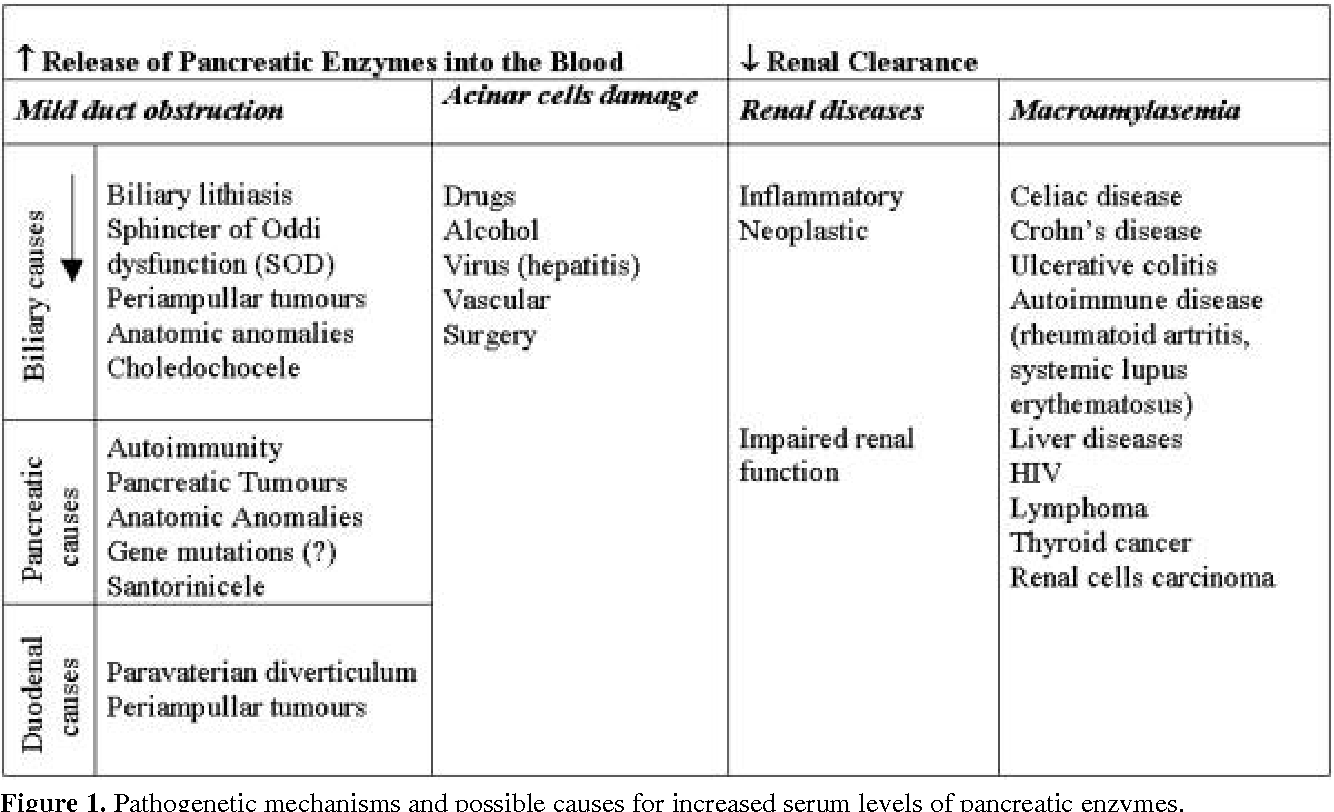 However, it does not necessarily mean that liver disease is worsening.
However, it does not necessarily mean that liver disease is worsening.
Itching is not unusual during pregnancy. It can result from hormonal changes or as the skin stretches. But, it can also result from a liver condition called intrahepatic cholestasis of pregnancy (ICP).
With ICP, bile acids do not flow properly, and they build up in the body, causing itching.
Symptoms of ICP include:
- itching, especially on the palms of the hands and soles of the feet
- dark urine
- jaundice
- pale stools
ICP typically disappears after delivery.
During pregnancy, the following may help manage itching:
- wearing loose-fitting clothes
- wearing cotton clothes
- taking cool baths
- avoiding using perfumes
- moisturizing
- avoiding spicy food, caffeine, and alcohol
Here are some common questions and answers about liver disease and itching.
Where does itching occur with liver disease?
It may occur anywhere in the body but notably in the palms of the hands and soles of the feet.
What kind of liver disease causes itching?
Itching is common in autoimmune liver diseases, such as primary biliary cirrhosis, primary sclerosing cholangitis, and obstructive biliary disease. It also occurs with cancer of the head of the pancreas, hepatitis, and drug-induced liver disease. However, it is less common with alcohol-induced liver disease and nonalcoholic fatty liver disease.
What are the signs that liver disease is getting worse?
Itching is not necessarily a sign of liver disease getting worse, but it may occur. As damage progresses, a person may experience confusion, easy bruising or bleeding, swelling in the abdomen, legs, and feet, and signs of jaundice, such as yellowing of the whites of the eyes.
There are many causes of pruritus, including some types of liver disease.
Experts do not know precisely why itching occurs with liver disease, although several theories exist. It is not a sign that liver disease is getting worse.
If a person has itching lasting more than 6 weeks, they should speak with a doctor.
Pruritus associated with cholestasis | Vyalov S.S.
Cholestasis is found in many diseases of the liver and biliary tract, which lead to extrahepatic biliary obstruction and/or intrahepatic impairment of bile excretion. In some patients, the most distressing and disturbing symptom associated with cholestasis is pruritus, which can vary in intensity, ranging from mild, moderate (resulting in sleep disturbance) to severe, in which the patient’s usual rhythm of life is completely disrupted.
The pathogenesis of pruritus in cholestasis has not been studied in detail, but several main hypotheses currently exist, including accumulation of bile acids and increased excitation of opioid receptors [1].
Bile acids
One theory suggests an increase in the level of bile acids in the skin of patients with cholestatic diseases, which leads to the appearance of pruritus. The observations of the followers of this theory demonstrate that a decrease in the amount of bile acids in the surface layers of the skin in this group of patients is associated with the intensity of itching, although the reliability of the methods used to determine this remains doubtful [2]. Other studies show the possibility that bile acid intake induces and exacerbates pruritus [3, 4].
Other studies show the possibility that bile acid intake induces and exacerbates pruritus [3, 4].
There are, however, three studies that do not contradict the main role of bile acids in pruritus:
- occasional improvement in pruritus despite ongoing cholestasis and high plasma bile acids [5];
- absence of pruritus in many patients with cholestasis and elevated plasma bile acids [5];
- obvious lack of correlation between the presence and severity of pruritus and the concentration of bile acids in the skin of patients with chronic cholestasis in most carefully conducted studies on this problem [6].
Moreover, cholestyramine and cholestipol, drugs used to treat cholestatic pruritus, also lead to a reduction in pruritus in patients with uremia and polycythemia vera, i.e., conditions not associated with retention of bile salts.
The relativity of the hypotheses is confused by the fact that elevated plasma bile acids due to hepatotoxicity affect pruritus to a greater extent than their direct effect on nerve endings [7]. Purified bile acids damage hepatocyte membranes, allowing cell contents (much of which can cause itching) to leak into the general circulation.
Purified bile acids damage hepatocyte membranes, allowing cell contents (much of which can cause itching) to leak into the general circulation.
Endogenous opioids
More and more importance is attached to the role of endogenous opioids in the pathogenesis of cholestatic pruritus [8]. Administration of opiates with μ-opioid agonist activity may exacerbate pruritus in healthy individuals, presumably through a central action. More importantly, endogenous opiate levels are increased (by an unclear mechanism) in patients with chronic liver disease [9, 10], and many studies show a reduction in cholestatic pruritus in patients treated with opioid receptor antagonists [8, 11-13].
Lysophosphatidic acid and autotaxin
Preliminary studies confirm the importance of the role of lysophosphatidic acid (LPA) in cholestatic pruritus [14]. LPA refers to phospholipids formed under the action of autotaxin, which splits off the choline group from lysophosphatidylcholine. Compared to controls, patients with cholestatic pruritus have significantly higher serum levels of exercise therapy and autotaxin activity. Moreover, injections of exercise therapy induce scratching responses in mice. These studies require confirmation but point to a potential role for autotaxin inhibitors as a therapeutic option.
Compared to controls, patients with cholestatic pruritus have significantly higher serum levels of exercise therapy and autotaxin activity. Moreover, injections of exercise therapy induce scratching responses in mice. These studies require confirmation but point to a potential role for autotaxin inhibitors as a therapeutic option.
Treatment
Treatment of the underlying liver and biliary tract disease may be an option for pruritus associated with cholestasis. In extrahepatic biliary obstruction in cases in which the main therapy is not possible, usually biliary drainage is very effective in stopping pruritus. In intrahepatic cholestasis, in cases in which the main therapy is not possible, some medications can be used, which can alleviate the symptoms of itching.
It is difficult to assess the efficacy of drug therapy for pruritus in clinical trials because the symptoms of pruritus are highly subjective and may wax and wane spontaneously. However, researchers now have state-of-the-art pruritus activity monitoring equipment that records scratching intensity independently of large body movements, thus allowing for behavioral methodology in clinical pruritus studies [15]. However, clinical studies are mostly small and use different scales to assess pruritus, so they are not comparable with each other to a limited extent [16].
However, clinical studies are mostly small and use different scales to assess pruritus, so they are not comparable with each other to a limited extent [16].
In mild cases, itching can be controlled with non-specific interventions such as warm baths, emollients, and sedatives. However, many of these remedies often do not work for moderate to severe itching or itching accompanied by excoriations. In such cases, the following treatment options are used.
Bile acid derivatives
Cholestyramine and cholestipol are effective first-line drugs in the treatment of moderate to severe cholestatic pruritus based on their favorable safety profile and clinical trial results [17]. There are a lot of clinical controlled studies on their use [16].
These preparations are not absorbed and contain basic polysterols that bind anions in the intestinal lumen. They also reduce bile acid levels by inhibiting bile acid reabsorption by about 90%. However, bile acid binding alone unfortunately cannot explain their effect, and more potent bile acid sequestrants (cholesevelam) are ineffective in cholestatic pruritus compared to placebo in controlled trials [18]. They also reduce pruritus in non-cholestatic disorders such as uremia and polycythemia vera, suggesting that they act on other mechanisms of pruritus.
They also reduce pruritus in non-cholestatic disorders such as uremia and polycythemia vera, suggesting that they act on other mechanisms of pruritus.
An effective dose of cholestyramine is in the range of 4 to 16 g/day. In addition, efficacy may be enhanced by pre- and postprandial dosing in patients with an intact gallbladder and increased secretion of itchogenic substances that may accumulate in the gallbladder during the night. However, adherence to treatment is a major problem in the use of bile acid derivatives. These drugs are relatively unpalatable, can cause constipation, and increase the absorption of various drugs, including digoxin, warfarin, propranolol, and thiazide diuretics.
Rifampicin
Some research results demonstrate a reduction in cholestatic pruritus at a dose of 300 to 600 mg of rifampicin per day [16, 19, 20]. Initially, it was thought that rifampicin could reduce pruritus by competing with bile acids for uptake in the liver, thus minimizing bile acid toxicity to hepatocytes. Conversely, rifampicin can induce microsomal enzymes that enhance 6-alpha-hydroxylation and consequently glucuronidation of toxic bile salts. However, these effects have not been confirmed and the interaction mechanism remains unclear.
Conversely, rifampicin can induce microsomal enzymes that enhance 6-alpha-hydroxylation and consequently glucuronidation of toxic bile salts. However, these effects have not been confirmed and the interaction mechanism remains unclear.
Although the toxicity of rifampicin was not found in these preliminary studies, caution should be exercised when using rifampicin in cholestatic conditions due to occasional hepatitis and severe idiosyncratic reactions [16].
Opioid receptor antagonists
Use of opioid antagonists such as injectable naloxone (0.4 mg bolus followed by 0.2 mcg/kg/min throughout the day), oral nalmefene (60 to 120 mg/day), oral naltrexone (from 12 to 5 to 50 mg/day) is often associated with partial relief of cholestatic pruritus [11, 16, 21–24]. This is illustrated by a controlled crossover study at 29patients, which showed a reduction in the need for scratching by 27% and a significant reduction in the perception of itching [21]. A similar study in 16 patients randomized to naltrexone or placebo showed that naltrexone was associated with a significant reduction in daytime pruritus symptoms (change in pruritus intensity -54% versus -8%) as well as at night (-44 % versus -7%) [22].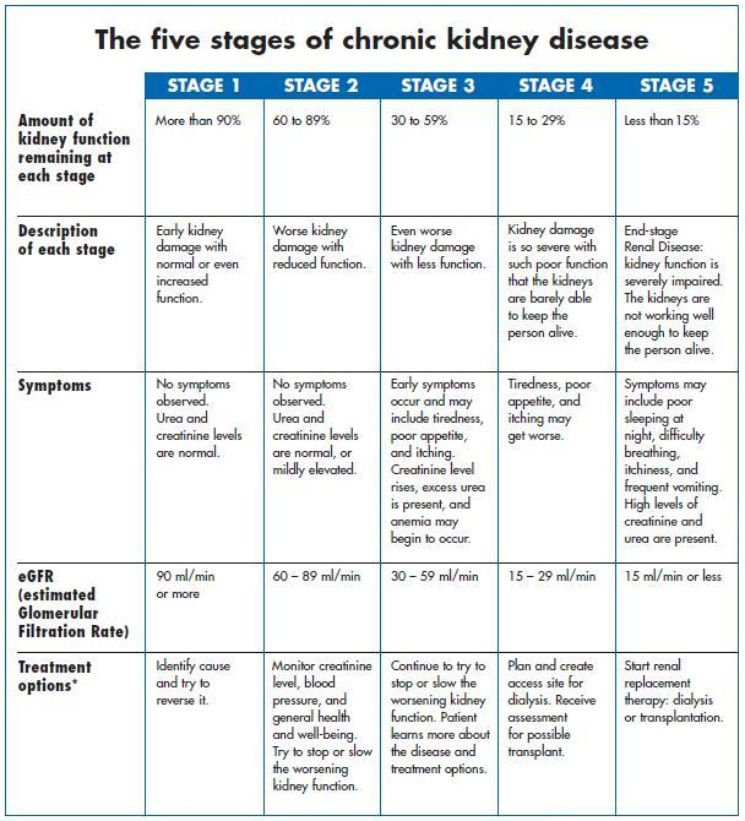 Persistent improvement was observed after 2 months. according to the results of the third placebo-controlled crossover study, including 20 patients [24]. 9patients noted a decrease in itching by more than 50%, and in 5 patients the symptoms of itching were completely stopped.
Persistent improvement was observed after 2 months. according to the results of the third placebo-controlled crossover study, including 20 patients [24]. 9patients noted a decrease in itching by more than 50%, and in 5 patients the symptoms of itching were completely stopped.
Opioid antagonists are generally well tolerated, with the exception of limited “withdrawal syndromes”, which most often resolve spontaneously within 2 days [24]. These problems are more evident with nalmefene, which is currently only available for experimental use [23]. The occurrence and intensity of the “withdrawal syndrome” can be reduced by careful initiation of intravenous administration (since naloxone is administered intravenously slowly at a rate of 0.002 μg / kg / min and the rate of administration is gradually increased until a therapeutic dose is reached) and switching to subsequent oral therapy [25 ]. In addition, opioid antagonists can lead to uncontrolled pain in patients with pain of various origins (eg, postherpetic neuralgia) [26]. By the time the role of endogenous opioids in cholestatic pruritus is better understood, the use of these drugs, including oral administration, will become more common in clinical practice.
By the time the role of endogenous opioids in cholestatic pruritus is better understood, the use of these drugs, including oral administration, will become more common in clinical practice.
Ursodeoxycholic acid
Ursodeoxycholic acid (UDCA) of natural origin is a bile acid administered exogenously, it changes the pool of bile acids to more hydrophilic ones [27, 28]. It remains unclear whether this effect is due to competition in intestinal absorption of endogenous bile acids or an increase in hepatic clearance of endogenous bile acids. UDCA is used in the treatment of certain forms of cholestatic liver disease, including primary biliary cirrhosis.
The effect of UDCA on pruritus, however, remains unclear [29]. Two large clinical trials in primary biliary cirrhosis, for example, showed no reduction in pruritus at UDCA doses of 13 to 15 mg/kg/day [30, 31]. In comparison, high-dose therapy (30 mg/kg/day divided into 3 doses) has shown significant improvement in pruritus symptoms in other studies [32]. In later studies, itching resolved in 6 of 7 patients in less than 1 month.
In later studies, itching resolved in 6 of 7 patients in less than 1 month.
Other means
Many other drugs can be used in the treatment of pruritus, but the number of studies conducted with their use is very limited and includes only a small number of patients.
Co-administration of colchicine and methotrexate significantly reduced pruritus in a controlled, double-blind study including 85 patients with primary biliary cirrhosis who kept an pruritus diary [33]. Phenobarbital has shown an effect in a number of studies [34, 35].
Clinical cases and small controlled studies support the potential efficacy of selective serotonin reuptake inhibitors. Sertraline (75 to 100 mg/day) was effective in a retrospective analysis of a group of patients with primary biliary cirrhosis who were part of a study of UDCA with and without methotrexate [36], as well as in a small randomized placebo-controlled crossover study of patients with pruritus in various liver diseases [37]. Paroxetine has shown good results in patients with severe non-dermatological pruritus (most of whom had non-liver causes of pruritus) [38].
Paroxetine has shown good results in patients with severe non-dermatological pruritus (most of whom had non-liver causes of pruritus) [38].
Phototherapy using ultraviolet (UV–B) has been effective in a number of studies [39–41]. The mechanism of pruritus reduction is not clear, although the hypothesis suggests an impairment of cutaneous sensitivity to pruritic substances or an alteration of the bile acid pool through the mobilization of skin bile acids. In our experience, phototherapy had no effect in more than 80% of patients with primary biliary cirrhosis who did not respond to cholestyramine therapy.
Several studies have shown improvement in pruritus symptoms after plasmapheresis in patients with cholestasis [42-44]. However, clinical experience is quite contradictory and heterogeneous. This technique is too multivariate to evaluate and difficult to apply for routine use. But plasmapheresis can play a role when other methods fail, and in patients with cirrhosis of the liver to reduce itching.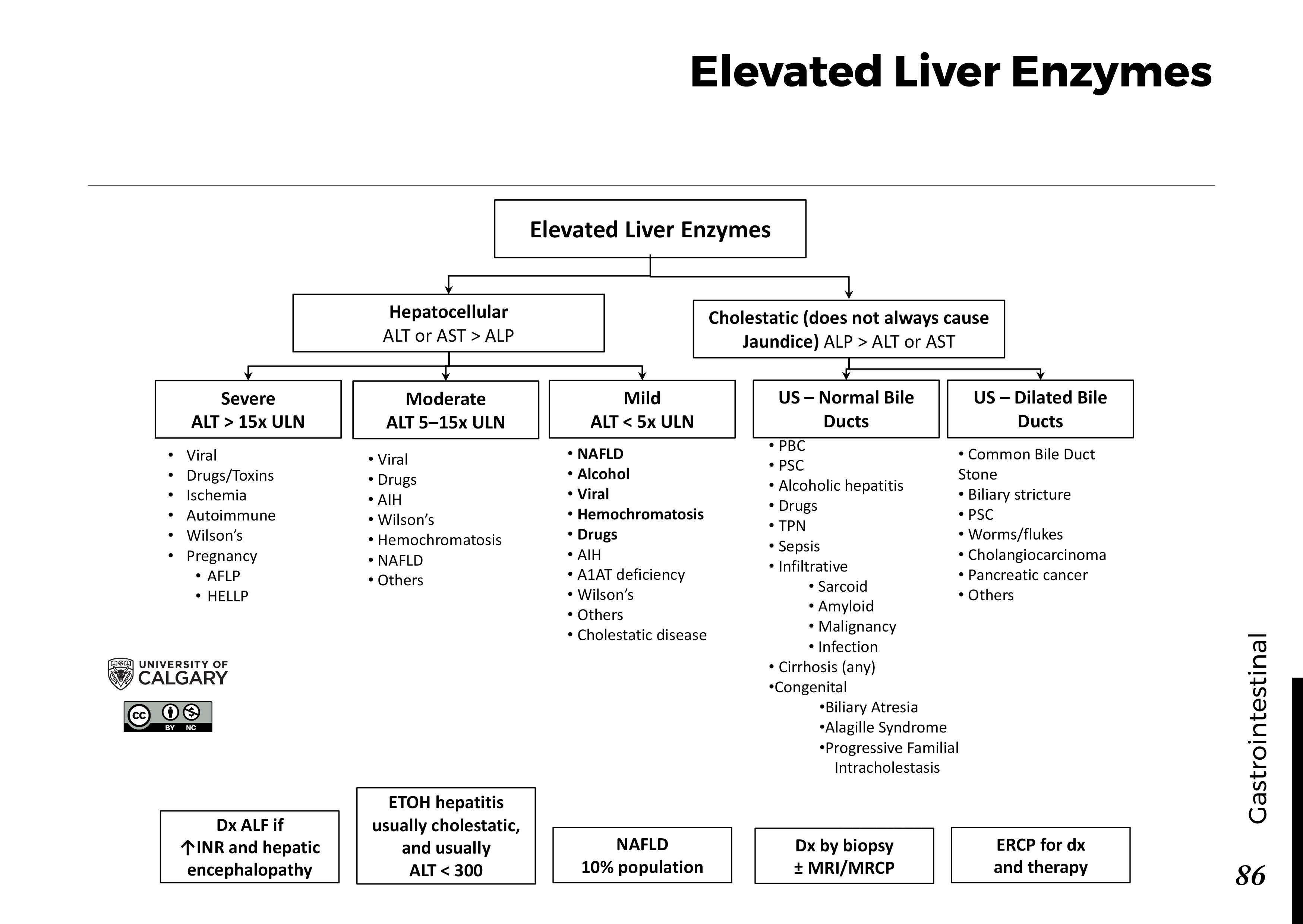
Propofol, a sedative anesthetic, was administered to 3 patients intravenously in subhypnotic doses [45]. There was a significant reduction in itching without disabling sedation. The proposed mechanism is associated with inhibition of the ventral and dorsal horns of the spinal cord, modulated by opioid-like ligands.
Androgens (such as norethandrolone, methyltestosterone, stanozolol) increase serum bile acids and worsen jaundice, and they paradoxically alleviate itch symptoms in patients with cholestasis [46]. The mechanism of this effect remains unclear, but many side effects limit the use of such drugs.
Delta-9-tetrahydrocannabinol relieves the symptoms of pruritus in some cases [47].
The molecular adsorptive circulatory system (hemofiltration devices) has also been effective in several series of observations [48–51].
Liver transplant
Severe pruritus refractory to other therapies may be a relative indication for liver transplantation in patients with severe cholestasis. A functioning liver transplant compensates for the underlying disease and contributes to the rapid resolution of itching.
A functioning liver transplant compensates for the underlying disease and contributes to the rapid resolution of itching.
American Association for the Study of the Liver Standards (AASLD, 2009)
The following approach is recommended for the treatment of pruritus in cholestasis associated with liver disease. Therapy is started with bile acid sequestrants. They are prescribed from 2 to 4 rubles / day before or after taking UDCA. In patients with pruritus refractory to treatment with bile acid sequestrants, rifampicin (150 to 300 mg bid) or oral opiate antagonists such as naltrexone (50 mg/day) may be used as the next step in therapy. Sertraline (75 to 100 mg/day) may be used when other methods fail (Fig. 1).
Conclusions and recommendations
1. Treatment of pruritus associated with cholestasis should primarily be focused on the treatment of the underlying disease of the hepatobiliary system. The tactics of treating extrahepatic biliary obstruction and intrahepatic cholestasis, the main conditions leading to the development of itching, are fundamentally different.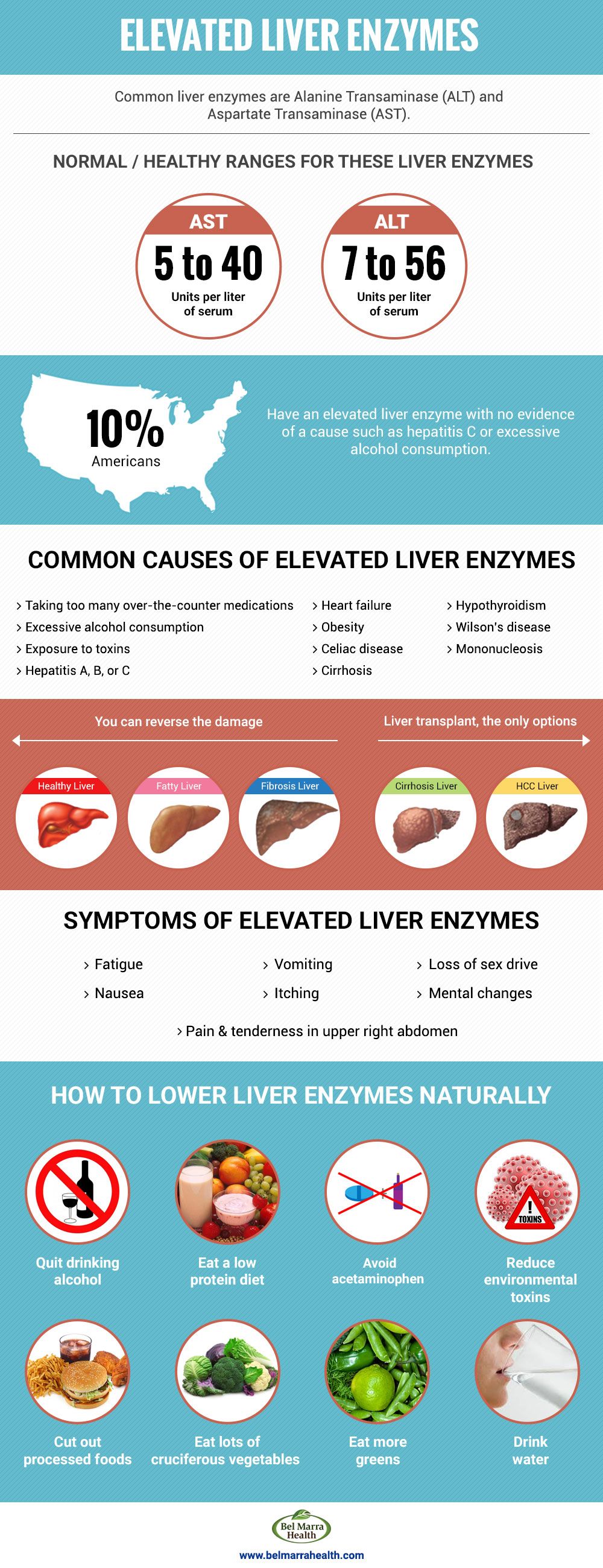
2. The optimal treatment for pruritus in cholestasis has not been definitively determined, although some studies have explored a range of treatment options (grade of evidence in brackets). The main criterion for choosing therapy is the severity and intensity of itching.
- General measures such as warm baths with or without antihistamines are recommended for mild pruritus (Class 2C).
- Cholestyramine or cholestipol are recommended to correct moderate to severe pruritus, or mild pruritus when general measures have failed (Grade 2B). An effective dose of cholestyramine is from 4 to 16 g / day. Efficacy may be enhanced when given before or after meals in patients with an intact gallbladder.
- Rifampicin 150 mg twice daily is recommended for the management of pruritus in patients who have not responded to cholestyramine and cholestipol (Class 2B).
It is sometimes used in first line therapy as well. In patients who have not responded to rifampicin, phenobarbital (90 mg once at night) is recommended, although drowsiness may occur during the first week of treatment (Class 2C).
- For the treatment of pruritus in patients with liver disease, UDCA at a high dose of 25–30 mg/kg/day divided into 3 doses is recommended. For the treatment of pruritus in patients with primary biliary cirrhosis, colchicine and methotrexate are recommended in addition to UDCA for non-responders (Class 2C).
- Opioid antagonists are recommended for the treatment of severe pruritus and in non-responders to other therapy (Class 2B).
Pathogenetic therapy of pruritus in patients with cholestasis
Author:
Professor of the Department of Gastroenterology of the Kharkov Medical Academy of Postgraduate Education, Doctor of Medical Sciences E.I. Sergienko
25.09.2019
PDF article
On June 13-14, a scientific and practical conference “The latest technologies in theoretical and clinical gastroenterology” was held in Dnipro. Within the framework of the event, 4 plenary sessions and 2 symposiums were held, dedicated to the latest achievements in the field of diagnostics and treatment of the pathology of the digestive system from the standpoint of evidence-based medicine. Professor of the Department of Gastroenterology of the Kharkov Medical Academy of Postgraduate Education, Doctor of Medical Sciences Elena Ivanovna Sergienko made a report “Practical aspects of the differential diagnosis of pruritus caused by cholestasis”.
– Pruritus is an infrequent, but painful manifestation that complicates the course of cholestatic liver diseases. Painful pruritus significantly reduces the ability to work and the quality of life of patients, leads to sleep disturbances, and causes depression. Differentiation of the cause of this symptom is of interest not only for dermatologists and gastroenterologists, but also for other specialists.
Skin itching without primary skin lesions may indicate somatic pathology and often accompanies diseases of the hepatobiliary system with cholestasis syndrome, and may also be present in chronic kidney disease, endocrine disorders (diabetes mellitus, hyper- and hypothyroidism, hyperparathyroidism), connective tissue diseases , blood (erythremia, paraproteinemia), mental disorders, malignant neoplasms, protozoal and helminthic invasions, as a side effect of taking medications.
Skin itching against the background of cholestasis can be observed in infectious, genetic, metabolic, autoimmune liver lesions that lead to extrahepatic biliary obstruction and / or intrahepatic impaired bile excretion (hepatocellular, canalicular, ductular types of cholestasis).
According to modern scientific research, central and peripheral mechanisms are important in the formation of pruritus in cholestasis: increased stimulation of skin receptors by pruritogens (bile acids, endogenous opiates, histamine, lysophosphatidic acid, cytokines), increased tone of opioid and imbalance of serotonin brain structures. These changes are possible against the background of genetic mutations leading to the development of cholestasis (mutations in the genes of proteins-transporters of hepatobiliary transfer of phosphatidylserine, phosphatidylcholine, bile salts), as well as violations of biochemical processes in liver cells (transmethylation, transsulfonation) and others (K. Tajiri, Y.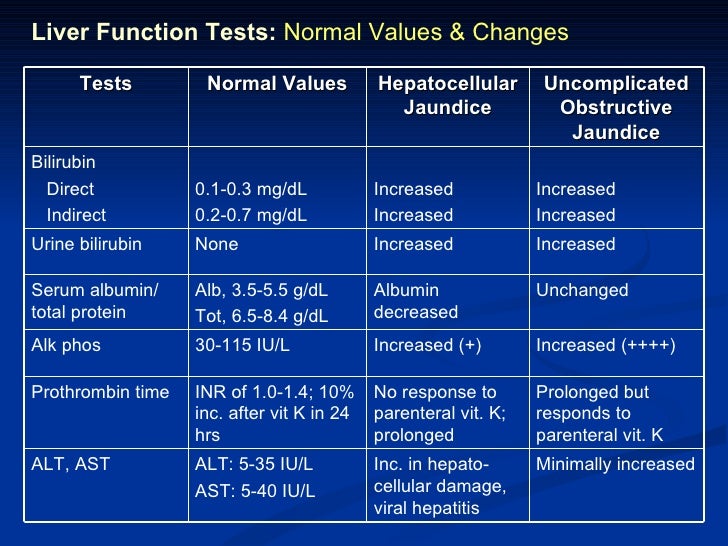 Shimizu, 2018).
Shimizu, 2018).
Skin itching against the background of cholestasis is not a pathognomonic manifestation of a specific disease, therefore, to determine the cause, it is necessary to study the history, clinical and laboratory data. One of the characteristic features of cholestatic pruritus is its circadian rhythm with the greatest intensity in the evening and night hours, as well as in warmth. In women, it increases during the progesterone phase of the menstrual cycle, during hormone replacement therapy and in late pregnancy, which indicates the role of female sex hormones in the pathogenesis of itching. Although pruritus is generalized in 25-50% of patients with cholestasis, its other specific feature is its localization in the back (in 70% of cases) or on the extremities, in particular, the palms and soles.
In the early stages of the disease, patients usually do not have primary skin changes. However, due to prolonged itching and constant scratching, redness of the skin, the appearance of linear urticaria, excoriated papules, cracks and crusts in the places of scratching and their infection are possible.
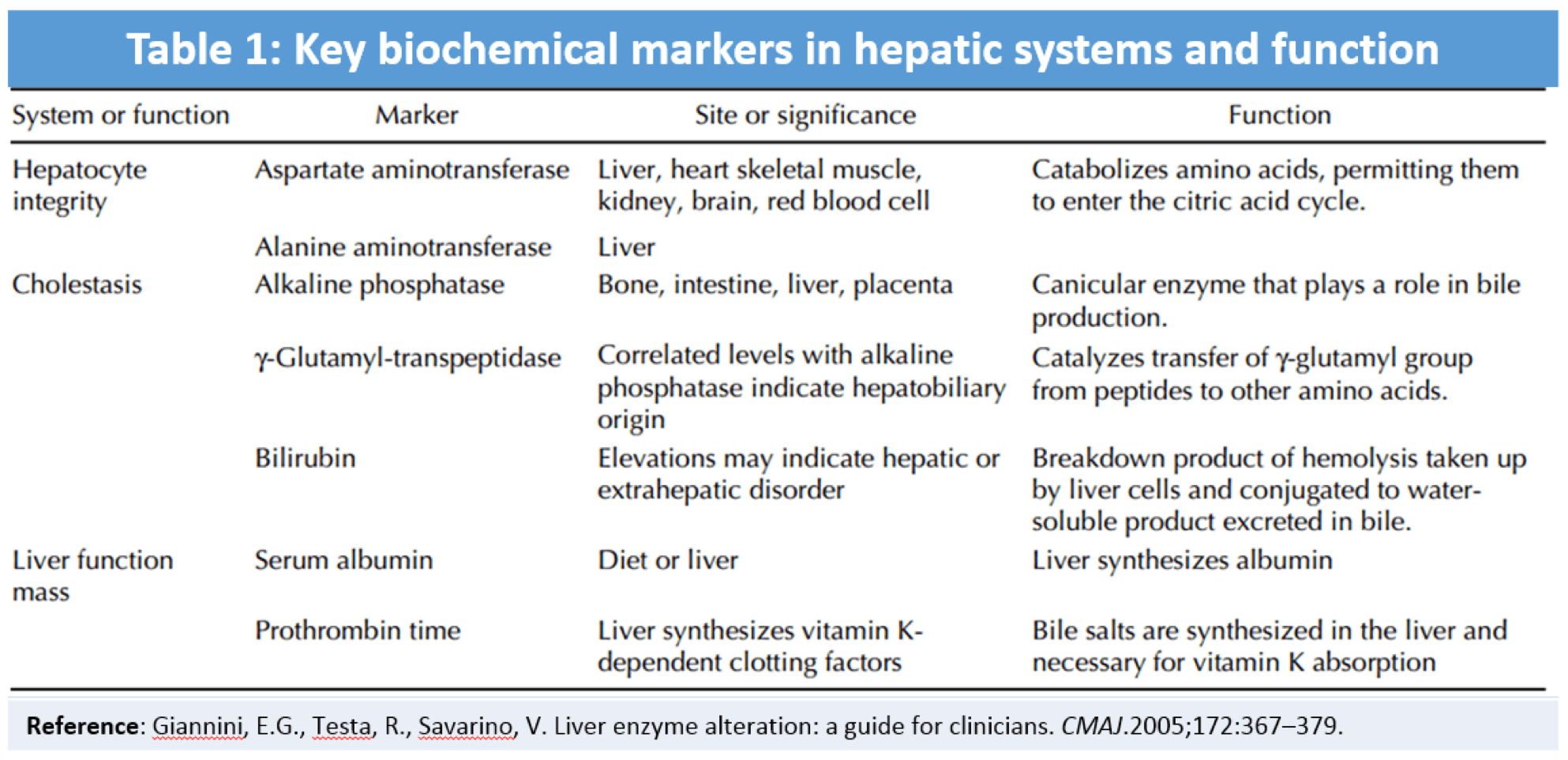
When choosing the optimal tactics for managing patients with hepatobiliary pathology and cholestatic pruritus, it is extremely important to differentiate extra- and intrahepatic cholestasis. At the first stage, the level of bilirubin and its fractions, urine urobilinogen, the activity of liver enzymes (ALT, AST), alkaline phosphatase, gamma-glutamyl transpeptidase, prothrombin time are determined, in some cases, the concentration of drugs in the blood is measured. Further, additional laboratory markers are used to clarify the etiology of the disease. So, if an autoimmune etiology of cholestasis is suspected, it is necessary to determine typical autoantibodies (ANA or NF, ASMA, LKM1). In primary biliary cirrhosis, antimitochondrial antibodies and the total level of class M immunoglobulins are determined. Serological diagnosis of hepatitis is necessary to confirm the infectious genesis of liver damage. Instrumental diagnostics must necessarily include an ultrasound examination of the liver and biliary tract to exclude a diffuse or focal process. In the absence of a clear understanding of the etiology, it is necessary to perform computed tomography with contrast, magnetic resonance cholangiopancreatography, endoscopic retrograde cholangiopancreatography, and diagnostic liver biopsy.
In the absence of a clear understanding of the etiology, it is necessary to perform computed tomography with contrast, magnetic resonance cholangiopancreatography, endoscopic retrograde cholangiopancreatography, and diagnostic liver biopsy.
Treatment of hepatobiliary pathology, accompanied by cholestasis syndrome and pruritus, involves the treatment of the underlying disease of the liver and biliary tract. With intrahepatic cholestasis, etiotropic and / or pathogenetic therapy is carried out. Unfortunately, a radical elimination of the cause is possible only with alcoholic liver disease and its viral diseases. An effective direction in the treatment of patients with extrahepatic biliary obstruction in situations where etiotropic treatment is impossible is biliary drainage.
Drug therapy for cholestatic pruritus includes the following areas: the elimination of pruritogens, the impact on the metabolism of pruritogens by transforming them into less toxic metabolites, the effect on opioid receptors, an experimental approach. In cholestasis syndrome with itching, the use of cholestyramine, rifampicin, naltrexone and sertraline is traditionally described, but the analysis of literature data indicates the absence of a rigorous evidence base for these drugs.
In cholestasis syndrome with itching, the use of cholestyramine, rifampicin, naltrexone and sertraline is traditionally described, but the analysis of literature data indicates the absence of a rigorous evidence base for these drugs.
Against the background of cholestatic liver diseases, a phased stepwise treatment of pruritus is recommended. Cholestyramine is considered the 1st line drug (level of evidence 2B). Despite being well tolerated, it has a number of side effects: it interferes with the absorption of vitamins A, D, E, K and some drugs, causes malabsorption, constipation, anorexia and digestive discomfort. Rifampicin belongs to the 2nd line of pharmacological treatment (level of evidence 2A). The main limitations when using rifampicin for the treatment of chronic cholestatic pruritus are hepatotoxicity with prolonged use of the drug (more than 2 weeks), a high risk of developing hemolytic anemia, renal failure, and thrombocytopenia. There is evidence of the effectiveness of µ-receptor antagonists in reducing the intensity of intractable pruritus, which made it possible to classify opioid receptor antagonists (naltrexone) as a 3rd line therapy (level of evidence 2B). Naltrexone is contraindicated in patients with drug dependence, severe liver failure. Sertraline, a selective serotonin reuptake inhibitor, is a 4th-line drug for the treatment of cholestatic pruritus (LE: 2C). In the absence of a positive effect from standard therapies, according to EASL recommendations, experimental therapies and early liver transplantation should be considered.
Naltrexone is contraindicated in patients with drug dependence, severe liver failure. Sertraline, a selective serotonin reuptake inhibitor, is a 4th-line drug for the treatment of cholestatic pruritus (LE: 2C). In the absence of a positive effect from standard therapies, according to EASL recommendations, experimental therapies and early liver transplantation should be considered.
The drug of choice for the pathogenetic treatment of patients with cholestasis is ursodeoxycholic acid (UDCA). It is a hydrophilic exogenous non-toxic tertiary bile acid, the content of which in the natural pool of human bile acids is only 4%. It has been proven that taking UDCA leads to an improvement in the secretory ability of hepatocytes, an increase in the passage of bile, a decrease in enterohepatic circulation of hydrophobic bile acids that have a toxic effect on hepatocyte membranes and biliary epithelium, a decrease in the lithogenic index of bile, an increase in gastric and pancreatic secretion, suppression of apoptosis and the production of pro-inflammatory cytokines. new (interleukins 1, 2, 6, interferon-γ), normalization of antigens HLA-DR on the surface of cell membranes, inhibition of the proliferative activity of fibroblasts associated with platelet growth factor, stabilization of cell membranes and antioxidant action (S.V. Morozov, Yu.A. Kucheryavy, 2015). A variety of mechanisms of action determine the variety of indications for prescribing a drug. UDCA is used for acute and chronic hepatitis (including autoimmune), toxic (including alcoholic) liver damage, primary sclerosing cholangitis, non-alcoholic fatty liver disease, primary biliary cirrhosis (before the formation of severe cirrhosis of the liver), cholestatic hepatosis of pregnant women, cystic fibrosis, gallstone diseases, for the lysis of X-ray negative cholesterol calculi in the gallbladder (no more than 15 mm in diameter) in patients with a functioning gallbladder. In cholestatic liver diseases of various origins, the average daily dose of UDCA is 12-15 mg/kg of body weight.
new (interleukins 1, 2, 6, interferon-γ), normalization of antigens HLA-DR on the surface of cell membranes, inhibition of the proliferative activity of fibroblasts associated with platelet growth factor, stabilization of cell membranes and antioxidant action (S.V. Morozov, Yu.A. Kucheryavy, 2015). A variety of mechanisms of action determine the variety of indications for prescribing a drug. UDCA is used for acute and chronic hepatitis (including autoimmune), toxic (including alcoholic) liver damage, primary sclerosing cholangitis, non-alcoholic fatty liver disease, primary biliary cirrhosis (before the formation of severe cirrhosis of the liver), cholestatic hepatosis of pregnant women, cystic fibrosis, gallstone diseases, for the lysis of X-ray negative cholesterol calculi in the gallbladder (no more than 15 mm in diameter) in patients with a functioning gallbladder. In cholestatic liver diseases of various origins, the average daily dose of UDCA is 12-15 mg/kg of body weight. Depending on the severity of the pathology, the daily dose can be increased to 20-30 mg / kg in 2-3 doses.
Depending on the severity of the pathology, the daily dose can be increased to 20-30 mg / kg in 2-3 doses.
The European standard for UDCA is Ursofalk by Dr. Falk Pharma GmbH. The drug is produced using innovative technologies in Germany and is used in many countries. The stability and high quality of the active substance of Ursofalk provides not only rapid relief of clinical and laboratory symptoms, but also a number of long-term consequences, such as slowing down the progression of the disease, improving the subjective status and quality of life, and reducing mortality (level of evidence A-B). Ursofalk is available in various dosage forms: suspension for oral use with a measuring cup (for children from birth and patients with difficulty swallowing), 250 mg capsules, 500 mg film-coated tablets. This allows each patient to choose the form of the drug that will be most convenient for him.
The pathophysiological mechanisms of itching are varied, and the use of drugs in accordance with stepwise algorithms and recommendations does not always lead to its regression, which indicates the insufficiency of modern pharmacological methods, the need to develop additional, more effective drugs. But in the treatment of liver diseases accompanied by cholestasis, prolonged use of Ursofalk is justified.
But in the treatment of liver diseases accompanied by cholestasis, prolonged use of Ursofalk is justified.
Prepared Victoria Bandaletova
Thematic issue “Gastroenterology. Hepatology. Coloproctology” № 3 (53), 2019
- Number:
- Thematic issue “Gastroenterology. Hepatology. Coloproctology» № 3 (53), 2019
07/06/2023
Gastroenterology Infusion of the probiotic Lactial® Germina Forte on clinical and laboratory indications and intestinal microflora in ailments on acute intestinal infections
Intestinal infectious diseases – the problem of infectious pathology is urgent. On the cob of a large-scale war on the risk of guilt
On the cob of a large-scale war on the risk of guilt
such ailments have grown significantly, and an increase in the number of cases of acute intestinal infections (GCI) is predicted. Threaten Zrostannia
viniknennya GKI priyatyat obmezheniya access to clean drinking water and hygiene, rebuvannya in places of crowding of people, temple
temperature dovkіllya, change in the term pridelnosti produktіv zhoshcho, after which the waking-ups of intestinal infections are signifi- cantly more
and it’s easier to expand in the usual middle ground ….
06/30/2023
GastroenterologyFunctional gastro-intestinal disorder and gastric secretion insufficiency: pathophysiological relationships and the role of enzyme replacement therapy
Functional gastro-intestinal and disorder (FGIR) – a group of ailments, such as chronic symptoms along the side of the herbal tract (abdominal pain, dysphagia, dyspepsia, diarrhea, fix that zduttya of the abdomen) for the visibility of the pathological state visible in case of obstezhennya. In our time, it is important that FGIR is blamed for the damage to interorgan communication between the brain and intestines (Fikree A., Byrne P., 2021)….
In our time, it is important that FGIR is blamed for the damage to interorgan communication between the brain and intestines (Fikree A., Byrne P., 2021)….
06/20/2023
Gastroenterology NPZP and gastrosafety: myth or reality?
12 May for the support of the Ministry of Health of Ukraine, the National Medical University named after. O.O. Bogomolets (m. Kiev), National University of Health Protection of Ukraine named after. P.L. Shupika (city of Kiev) held a symposium “Management of pain and stress disorders”, in the program of which Bulo presented a wide range of additional ideas related to the control of pain and stress. Of particular interest is the associate professor of the Department of Clinical Pharmacy and Clinical Pharmacology of the Vinnitsa National Medical University named after.